



Medical Research
Disease Specific

Medical Specialists
Deals with all diseases within the specialty which often is derived from an organ(s) or body system.
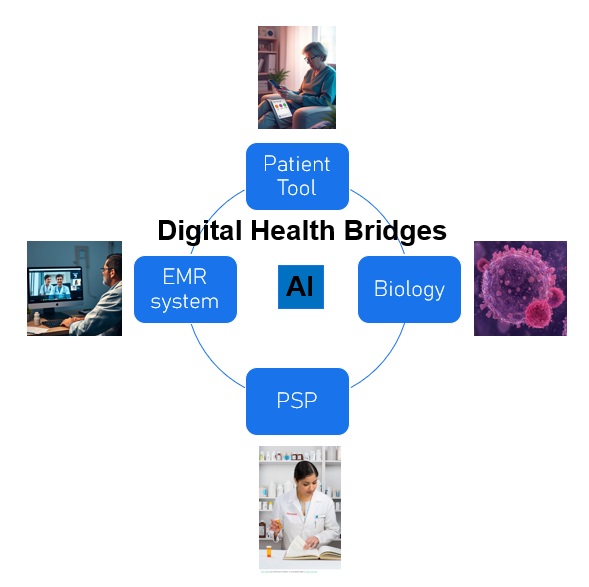
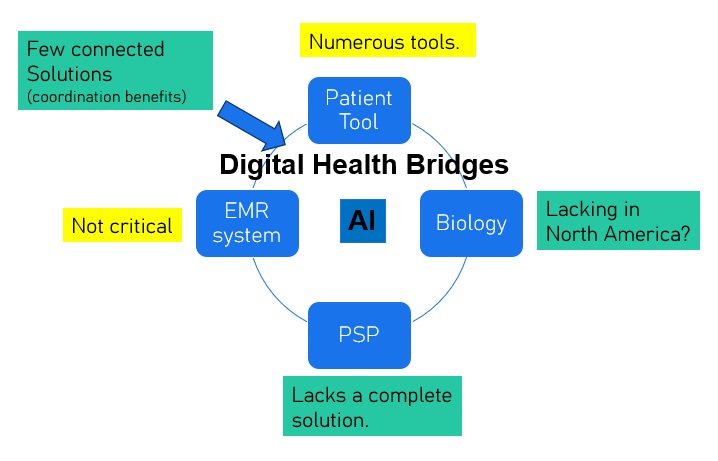
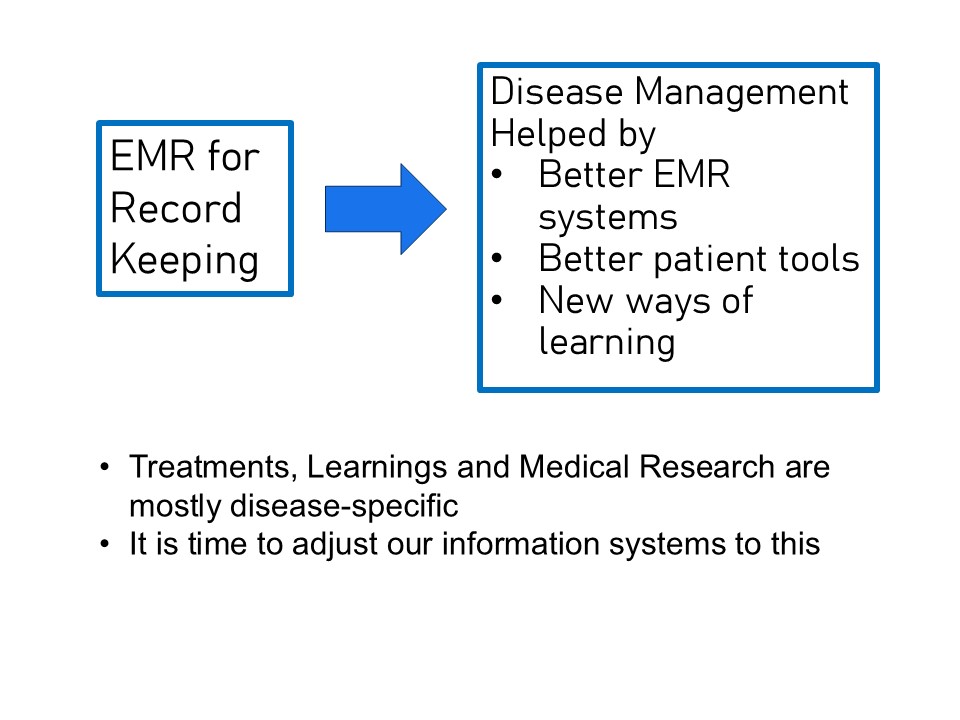
EMR Systems
Some systems are preferred or better suited for some specialties. But generally, they can be used to support most diseases and illnesses.




In The Clinic
• AI assist is used to produce your notes and for decision support.
• The EMR system is prepopulated with information from the patient before any interaction.
• AI will help schedule patients according to estimated time. Patients schedule their own visits.
• Helped by AI, relevant information is shown in a disease dashboard to make it easier to see key data in a snapshot. This may include data entered by patients before the visit, between visits, from the app, or by monitoring devices.
• Your system will enable you to send an AI-generated summary of the visit and the treatment plan to the patient.
• The system can generate suggested prescriptions for you to approve based on the situation, your history of prescriptions, and your preferences. The patient automatically gets a copy of the prescribed information. The same applies for lab requisitions. Both may integrate forward with the pharmacy and the lab for convenience
• The system may suggest useful information for the patient, which can be directed by simply ticking a box. You may set up your system to send this information to all patients with specific conditions. AI will help you organize this over time.
• Additionally, if you think any type of longitudinal data would be useful, you can discuss its collection and get an agreement. Further information and instructions are sent to the patient by ticking a box in your system. The system will allow you to customize the the collection.
• The EMR system is prepopulated with information from the patient before any interaction.
• AI will help schedule patients according to estimated time. Patients schedule their own visits.
• Helped by AI, relevant information is shown in a disease dashboard to make it easier to see key data in a snapshot. This may include data entered by patients before the visit, between visits, from the app, or by monitoring devices.
• Your system will enable you to send an AI-generated summary of the visit and the treatment plan to the patient.
• The system can generate suggested prescriptions for you to approve based on the situation, your history of prescriptions, and your preferences. The patient automatically gets a copy of the prescribed information. The same applies for lab requisitions. Both may integrate forward with the pharmacy and the lab for convenience
• The system may suggest useful information for the patient, which can be directed by simply ticking a box. You may set up your system to send this information to all patients with specific conditions. AI will help you organize this over time.
• Additionally, if you think any type of longitudinal data would be useful, you can discuss its collection and get an agreement. Further information and instructions are sent to the patient by ticking a box in your system. The system will allow you to customize the the collection.

For Research
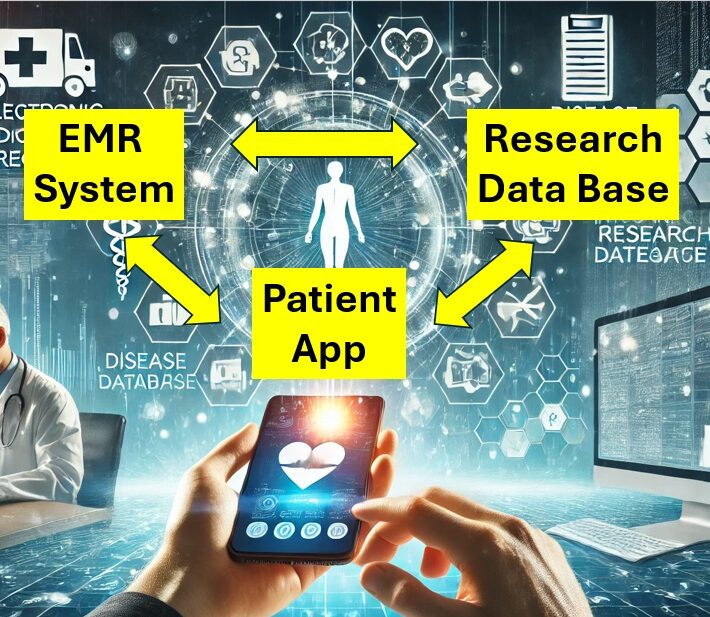
In a de-identified database, researchers will now have the ability to longitudinally connect structured treatment data (prescriptions) unstructured data from EMR systems, patient generated data, automatically generated app and phone data, and biological data. Traditionally it has been difficult to combine data in this way if it has been collected at all.
• Improved data collection in EMR systems
• “Prescribed” (physician-initiated) collection of data directly from patients.
• Automated collection of data from a disease management app.
• Donation of tissue or other biological samples. By patients.
• Improved data collection in EMR systems
• “Prescribed” (physician-initiated) collection of data directly from patients.
• Automated collection of data from a disease management app.
• Donation of tissue or other biological samples. By patients.